FREE Consultation
What happens if I’m not suitable for Laser Eye Surgery?
At London Vision Clinic, we are able to treat around 98% of the patients we see using one of our Laser Eye Surgery treatments; however, Laser Eye Surgery may not be suitable for a small number of patients. This can be due to the severity of their prescription, the shape of their eyes, or the health of the corneas.
But that doesn’t necessarily mean that new and improved vision is out of your reach.
In fact, several alternative options may help you to see more clearly. Of these, phakic intraocular lens implantation is one of the most common.
What should I expect during the procedure?
Traditionally, cataract surgery and other lens implant procedures have been performed on one eye at a time, with an interval of at least a few days between eyes. The historical justification for this was to minimise the risk of serious complications occurring in both eyes. However, following research by the International Society of Bilateral Cataract Surgeons (ISBCS), and the accumulation of several large-scale studies, it was concluded that treatment of both eyes on the same day does not statistically increase the risk of bilateral serious complications. In fact, this approach may even reduce the risk of complications.
Furthermore, there are additional benefits to performing treatment on both eyes at the same time. These include overall faster outcomes and recovery times, fewer clinic visits, and less time off work.
Whether you have treatment on both eyes on the same day will be decided between yourself and your surgeon. In some cases, your surgeon may recommend that you have each eye treated on separate days. The relevant risks and benefits of immediate versus delayed sequential surgery will be fully discussed with you before a decision is made.
After your ICL treatment, you will stay at the clinic for between 30 and 60 minutes before undergoing your final checks. This will include eye pressure and lens position reviews. You will also be provided with eye drops that should be applied for 1-2 weeks after your surgery. During your recovery, you will need to attend several follow-up appointments at the clinic to ensure everything is going as planned.
What are the benefits of ICLs?
- The procedure is reversible. Should your vision change, you can have laser treatment to refine your vision. Alternatively, the lens implants can be replaced or removed if required.
- It can successfully treat a wider range of prescriptions.
- May be able to treat patients with corneal conditions that might not qualify for Laser Eye Surgery (such as keratoconus).
What are the risks of ICLs?
- ICL surgery is more invasive than Laser Eye Surgery, which means it carries greater risks. Minor risks include a short-term increase in eye pressure, and inflammation inside the eye.
- Expected side effects are similar to laser eye surgery and include mild irritation and halos at night that usually subside over time.
- Most patients experience only minimal discomfort and are able to go back to work within a few days of the procedure.
Implantable Collamer Lens
Phakic Intraocular Lens Implantation, also known as Implantable Collamer Lens (ICL) Surgery
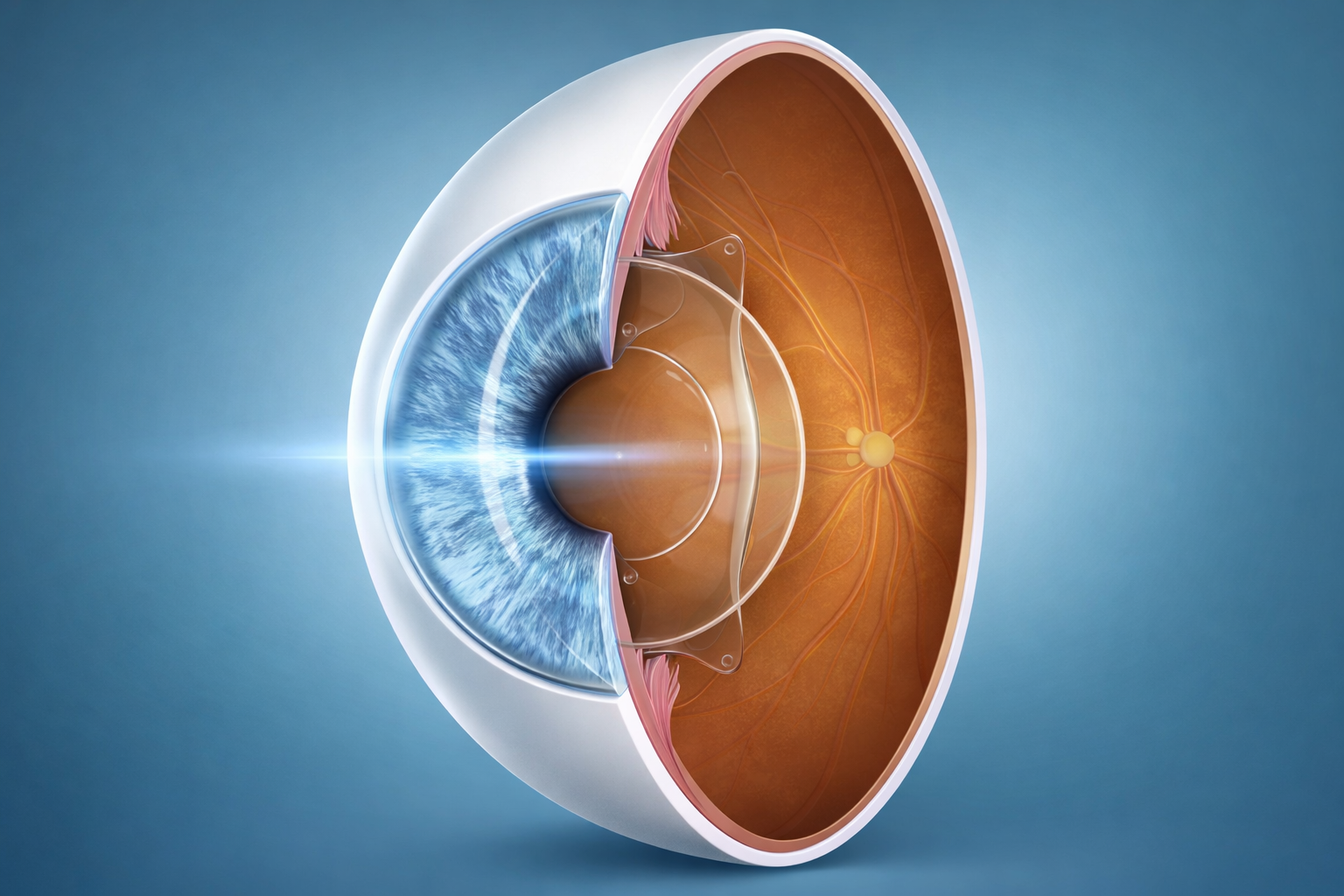
Also known as Implantable Collamer Lens (ICL) surgery, this procedure involves implanting a small, artificial lens into the eye. This lens sits behind the iris and in front of the eye’s natural crystalline lens.
In 1997, the ‘V4’ ICL model was approved for use in the UK, and quickly became the go-to treatment option for patients who were not candidates for Laser Eye Surgery. However, these lenses were associated with an increased risk of cataract formation post-surgery. A few years later, a new and improved model, featuring a small hole in the centre of the lens, was introduced. These lenses improved safety and reduced the risks associated with ICL surgery.
To date, millions of ICLs have been implanted worldwide.
ICL Surgery can be suitable for a wide range of prescriptions: It is available for treating myopia (short-sightedness) between -0.50 D and -20.00 D, hyperopia (long-sightedness) between +0.50 D and +10.00 D, and astigmatism up to +6.00 D. The lens is also available in a range of sizes to accommodate a range of eye sizes.
ICL Surgery may be offered to you if it is not possible to fully correct your refractive error with Laser Eye Surgery. This alternative treatment can also be performed alongside Laser Eye Surgery on the surface of the eye to correct any residual refractive error which may not have been fully corrected by the intraocular lens, a technique called Bioptics.
The most advanced and accurate method for ICL sizing is by using the Artemis Insight 100 VHF digital ultrasound scanner. This technology allows us to directly measure the area inside the eye, behind the iris, where the lens will be sitting. This provides more accurate information for ICL sizing than simply estimating the size based on external measurements. Using the most advanced methods helps to minimise the risk of complications or needing an ICL exchange surgery.
How many appointments will I need?
How many appointments you will need can depend on several factors. Perhaps the most important is the severity of your prescription.
The higher your prescription, the greater the power of the lens required to correct it your refractive error. This can affect how many appointments you need and the pattern of your aftercare.
If you are short-sighted, the ICL used in your treatment will feature a small hole in the centre to allow fluid to flow around the lens inside the eye. However, these lenses are generally not suitable for long-sighted patients. In these cases, a very short laser procedure will be performed to create a small hole in the iris to allow fluid to flow through. This will be performed by a surgeon and generally takes around one minute per eye.
How does the process differ from laser eye surgery?
The testing and screening process for ICL surgery is largely the same as the protocol for Laser Eye Surgery candidates, with the addition of a full bitreous and retina examination. It is essential to assess the health of the peripheral retina, which provides side-vision. State-of-the-art wide-field imaging allows us to monitor for certain retinal pathologies that can affect the success of phakic intraocular lens surgery.
What to expect after ICL surgery
Most patients will be able to return to many everyday activities just 24 hours after their ICL surgery. However, there are some important things to note. For example, you should avoid rubbing your eyes or getting anything in them. Activities such as swimming and intense exercise should be avoided. If your eyes are stable at one week post-surgery, your surgeon will sign you off to resume most activities.
You will be required to attend several check-ups at your clinic for the first year to monitor your recovery. After your one-year follow-up visit, it is important to continue to attend annual check-ups with an eye care provider. These appointments will include a dilated retinal exam to monitor the positioning of the lens inside the eye and the overall health of the eye, including the back of the cornea, iris, lens, and retina.
As also seen with Laser Eye Surgery, a small prescription may remain after ICL implantation. This residual refractive error tends to be very small, but can generally be addressed in several ways. After ICL surgery there are no restrictions on the type of glasses or contact lenses a patient can wear. You can also explore laser refractive surgery to treat any residual prescription (assuming you have no corneal conditions which precluded you from laser treatment in the first place).
Professor Reinstein explains what sizing methods are used for ICL surgery at London Vision Clinic
The most advanced and accurate method for ICL sizing is by using the Artemis Insight 100 VHF digital ultrasound scanner. This technology allows us to directly measure the area inside the eye, behind the iris, where the lens will be sitting. This provides more accurate information for ICL sizing than simply estimating the size based on external measurements. Using the most advanced methods helps to minimise the risk of complications or needing an ICL exchange surgery.